Functional indices of cardiac perdormance in adolescents with different rates of physical development
Фотографии:

ˑ:
Dr.Med., Professor A.L. Korepanov
Sevastopol State University, Sevastopol
Keywords: adolescents, physical development, functional state of myocardium.
Introduction. The advancement of the sports science and practice is founded on the conception of human motor activity age-related evolution and is implemented on the basis of anthropic educational technologies [9]. Due to popularity of sports and healthy lifestyle more and more teenagers are being engaged in it. The marked heterochronicity of development of physiological systems increases the probability of functional deviations in the cardiac performance in adolescents during sport trainings. The number of cases of pediatric cardiac pathologies has recently increased [4; 11]. A disease that is not promptly diagnosed may cause cardiac and vessel pathological changes developed in the training process [3]. Sport trainings cause more rapid morphological and functional changes in the cardiovascular system of adolescents than in the one of adults [1]. The cardiac remodeling processes which develop during training sessions in adolescents may cause pathological cardiac transformation, which leads to the development of organic cardiovascular disease [12]. The problem of sudden death remains urgent: 1 out of 50 thousand young athletes dies during sport training due to heart diseases such as cardiomyopathy, carditis, arteries anomalies, etc., that have not been promptly diagnosed [13].
The issue of peculiarities of hemodynamics in adolescents with different levels of physical development – accelerants (Ac), normodants (No), retardants (Re), is poorly covered in the literature. Single studies and the author’s personal results indicate different adaptation reserves and homeostasis supporting mechanisms, different levels of somatic health and physical working capacity for Ac, No, and Re [5, 6, 8]. It is of practical importance to study adolescent's cardiac functionality before he/she starts doing sports taking into account the differences in the rates of physical development. The study consists in using the received data on cardiac performance characteristics to elaborate training process optimization technologies and to prevent cardiac pathological transformation in adolescents.
Objective of the research was to assess cardiac performance in adolescents with different rates of physical development using the method of polycardiography.
Methods and structure of the research. Subject to the study were 160 adolescents – boys at the age of 13-14 years. The research was carried out in the Sevastopol State University Laboratory of Physiology. The respondents were divided into groups with accelerated (Ac), normal (No), and retarded (Re) physical development based on the formerly indicated height standards for adolescents from Sevastopol [7]. The adolescents whose height was within the limits of М±σ were referred to the No-group, the ones with the height exceeding М+σ – to the Ac-group, those with the height lower than М–σ – to the Re-group.
The study of cardiac performance characteristics (cardiac cycle phase structure indices and myocardial function indices) was carried out by means of computer polycardiography using cardioanalyser MTC-30 (city of Krasnodar) [10]. There were registered 3 ECG leads according to W. Einthoven's system, phonocardiogram (PhCG), and carotid artery differential sphygmogram (DSG). The automated interpretation of ECG, PhCG and DSG was conducted in accordance with cardiac cycle phases. The indices of cardiac cycle phase structure were determined after recoding the signals (6.3 s) and entering the data of testee's sex, age, height, body weight and arterial pressure (AP) indices into the program. The following indices of cardiac cycle phase structure were determined in accordance with the operating algorithm of the program: asynchronous contraction phase, isometric contraction phase, tension period, ejection period, acoustic systole, total systole, and aortic open valves period. The following indices of myocardial contractility and myocardial functional status were determined: mean rate of ventricular pressure rise, myocardial strain index, mean acceleration of left ventricular pressure rise, acceleration of arterial pressure rise, cardiac contractile reserve, cardiac mobilization rate, experienced stress level, adaptation potential of the cardiovascular system. The materials were statistically processed by means of STATISTICA for WINDOWS 6.0.
Results and discussion. The study revealed essential differences in myocardial contractility in adolescents with different levels of physical development (Tab. 1, Fig. 1).
Table 1. Cardiac performance indices (М±m) for accelerants, normodants, and retardants
|
Index |
Accelerants (n=33) |
Normodants (n=83) |
Retardants (n=44) |
Total (n=160) |
|
Asynchronous contraction phase, ms |
51,1±1,3 |
47,9±1 |
46,7±0,9 |
48,3±1,1 |
|
Isometric contraction phase, ms |
27,8±0,9 |
27,5±1,3 |
26,8±1 |
27,4±1,1 |
|
Tension period, ms |
77,3±1 |
75,45±1,1 |
73,54±1 |
75,31±1 |
|
Ejection period, ms |
243,1±2,2 |
245,2±2,5 |
250,3±2,8 |
246,2±2,4 |
|
Acoustic systole, ms |
308,9±2,7 |
312,2±2,1 |
314,3±2,4 |
311,4±2,5 |
|
Total systole, ms |
317,4±3,2 |
320,5±3 |
322,8±3,5 |
320,5±3,3 |
|
Aortic open valves period, ms |
287,3±2 |
286,3±2,4 |
287,6±2,8 |
286,9±2,4 |
|
Myocardial strain index, % |
24,4±0,6 |
23,8±0,4 |
23±0,5 [2] |
23,7±0,4 |
|
Mean rate of ventricular pressure rise, mmHg/s |
2223,8±50,1 |
2119,5±40,8 |
2168,3±40,5 |
2154,4±40,7 |
|
Mean acceleration of pressure, st. un. |
1106,9±28 [1]
|
949,9±25 |
939,4±27 [2] |
979,4±26 |
|
Acceleration of AP rise, st. un. |
1483,9±30 [1] |
1260,9±41
|
1246,1±35 [2] |
1302,9±33 |
|
Cardiac contractile reserve, st. un. |
590,7±15 [1] |
652,7±18
|
666,2±20 [1,2] |
643,6±17
|
|
Cardiac mobilization rate, st. un. |
1,5±0,02 [1] |
1,4±0,04
|
1,36±0,04 [2] |
1,41±0,03 |
|
Stress level, st. un. |
1,73±0,04 [1] |
1,66±0,03
|
1,55±0,05 [1,2] |
1,64±0,04 |
|
Adaptation potential, st. un. |
1,8±0,02 [1] |
1,71±0,06
|
1,61±0,04 [2] |
1,64±0,04 |
Note: [1] – p<0, 05 when compared with the indices of normodants; [2] - p<0,05 when compared with the indices of accelerants.
The parameters of cardiac cycle analysis (asynchronous contraction phase, isometric contraction phase, tension period, ejection period, acoustic systole, total systole, and aortic open valves period) did not display any significant inter-group differences; yet the tendency to the phase of isometric contractility increasing in Ac in comparison with Re was detected, which correlates with the general dynamics of contractility decrease in Ac.
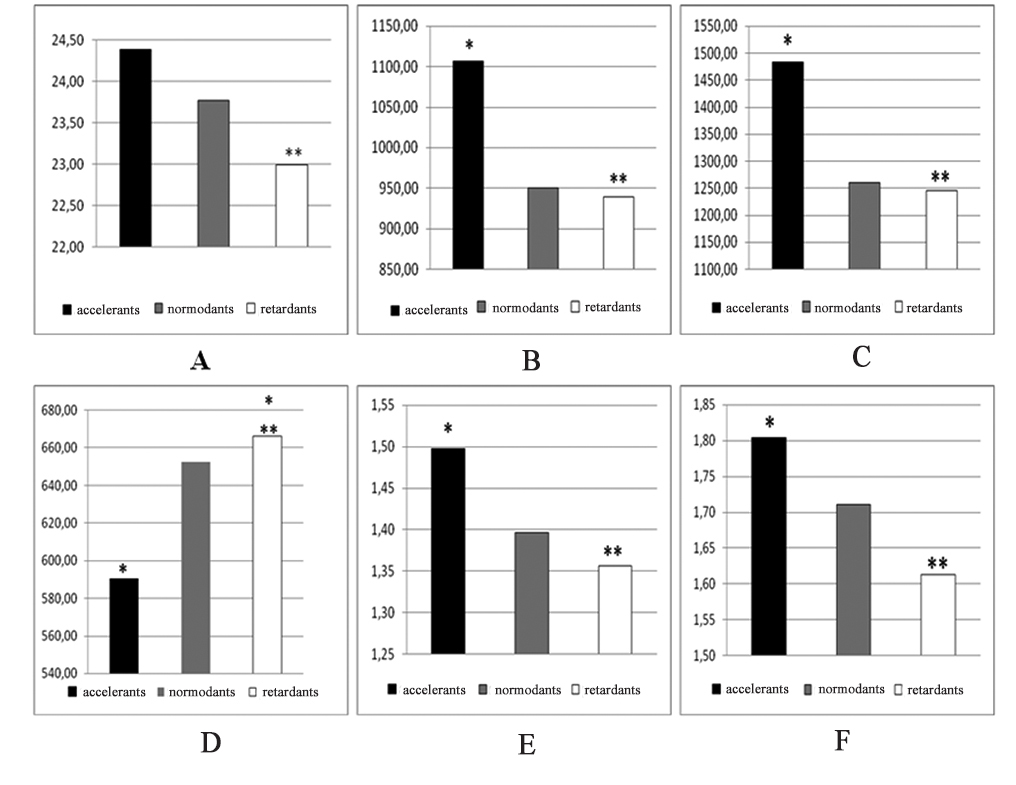
Figure 1. Comparative parameters of myocardial contractility in accordance with the indices of polycardiography in accelerants, normodants, and retardants
A – myocardial strain index (%), B – average acceleration of isometric rise (st. un.), C –acceleration of AD rise (st. un.), D – cardiac contractile reserve (st. un.), E – cardiac mobilization rate (st. un.), F – adaptation potential of cardiovascular system (st. un.). Black rectangles – accelerants, gray rectangles – normodants, white rectangles – retardants.
Note: * – р < 0.05 when compared with the indices of normodants; ** – р < 0.05 when compared with the indices of accelerants.
Essential intergroup differences were seen from more significant indices of myocardial contractility. Thus, the myocardial strain index was significantly higher in Ac versus Re, which reflects the decrease of myocardial contractility function in Ac. The adaptation potential of the cardiovascular system, that characterizes the strain of adaptive-regulative systems of the body in general and the rate of myocardium function economization [2], was significantly higher in No and Re as opposed to Ac (the lower the index, the higher the rate of adaptation).
The cardiac mobilization rate as the most objective index of myocardium workload that reflects the oxygen uptake rate and the degree of correspondence of cardiac performance to the current energy expenditure rate was the highest in Ac and the lowest in Re. The decrease of contractility and functional reserves in Ac was also marked in accordance with the index of cardiac contractile reserves: they were registered as significantly lower in Ac as opposed to No and Re. Extra cardiac mobilization in Ac that may be associated with an increase of post-workload by the peripheral vascular resistance was reflected in the increase in the acceleration of the arterial pressure rise and in the mean acceleration of left ventricular pressure rise, as compared with No and Re. Ac experienced more stress (in accordance with the stress rate index) than the adolescents from two other groups.
References
- Avdeeva T.G., Vinogradova L.V. Vvedenie v detskuyu sportivnuyu meditsinu [Introduction to children's sport medicine]. Moscow: GEOTAR-Media publ., 2009, p. 40.
- Baevskiy R.M., Kirillov O.I., Kletskin S.Z. Matematicheskiy analiz izmeneniy serdechnogo ritma pri stresse [Mathematical analysis of heart rate changes during stress]. Moscow: Nauka publ., 1984, 221 p.
- Balykova L.A. Izmeneniya serdechno-sosudistoy i immunnoy sistem u yunykh sportsmenov: polozhitel'nye effekty L-karnitina [Changes in cardiovascular and immune systems in junior athletes: positive effects of L-carnitine]. Pediatriya.«Consilium Vedicum», 2014, no. 4, pp. 20-24.
- Dolgikh V.V., Prokhorova Zh.V., Fomina N.A. Rol psikhoemotsional'nykh i sotsial'nykh faktorov v razvitii essentsial'noy arterial'noy gipertenzii u podrostkov [Role of psycho-emotional and social factors in essential hypertension development in adolescents]. Pediatriya, 2011, no. 5, pp. 25-28.
- Korepanov A.L. Differentsial'naya kharakteristika morfofunktsional'nykh parametrov podrostkov s raznym urovnem fizicheskogo razvitiya [Differential characteristics of morphofunctional characteristics of adolescents with different levels of physical development]. Vestnik fizioterapii i kurortologii. Spetsial'ny vypusk [Bulletin of physiotherapy and balneology], 2007, no. 2, pp. 33-40.
- Korepanov A.L. Differentsial'noe issledovanie fizicheskoy rabotosposobnosti i energoobmena u podrostkov [Differential study of physical working capacity and energy exchange in adolescents]. Arkhiv klinicheskoy i eksperimental'noy meditsiny, 2006, vol. 15, no. 1, pp. 28-33.
- Korepanov A.L. Issledovanie dvigatel'noy reaktsii u podrostkov [Motor response in adolescents]. Vestnik fizioterapii i kurortologii. Spetsialny vypusk, 2007, pp.48–52.
- Krukovich E.V., Luchaninova V.N., Nagirnaya L.N. Dinamika fizicheskogo razvitiya detey g. Vladivostok [Dynamics of physical development of children in Vladivostok]. Pediatriya, 2003, no. 6, pp. 89 – 96.
- Lubysheva L.I., Zagrevskaya A.I. Kineziologicheskiy podkhod kak metodologiya sovremennoy sportivnoy nauki i praktiki [Kinesiological approach as methodology of modern sports science and practice]. Teoriya i praktika fiz. kultury, 2015, no. 12, pp.3-5.
- Polikardiometr MTK-30. Instruktsiya po ekspluatatsii [Polycardiometer ITC-30. User's manual]. Krasnodar: Elektropribor publ., 2003, 150 p.
- Popov S.V., Bokova S.I. Sostoyanie serdechno-sosudistoy sistemy u detey shkol'nogo vozrasta, rozhdennykh pozdnenedonoshennymi [Сardiovascular status of premature school-age children]. Perinatologiya i pediatriya, 2012, no. 4, pp. 72-76.
- Basavarajaiah S. Physiological left ventricular hypertrophy or hypertrophic cardiomyopathy in an elite adolescent athlete: role of detraining in resolving the clinical dilemma. Br. J. Sports Med. 2006, no. 40, pp.727–729.
- Maron B.J. Strategies for assessing the prevalence of cardiovascular sudden deaths in young competitive athletes. Int J Cardiol., 2014, vol. 72, pp.173-369.
Corresponding author: akorepanov2006@rambler.ru
Abstract
Objective of the present research was to conduct a comparative analysis of cardiac performance in adolescents with different rates of physical development.
Subject to the study were 160 adolescents – boys at the age of 13-14 years. The functional indices of cardiac performance and myocardial contractility were studied using computer polycardiography.
The results displayed that the functional status and the myocardial contractility ability depend on the rates of physical development. The myocardial performance of accelerants is less effective, which is confirmed by the increase of the cardiac mobilization rate, the decrease of its contractility reserve, and adaptive capability. The revealed regularities must reflect the decrease of the body's adaptive resources in the adolescents with high physical development rates.

