
Features of muscles bioelectrical activity when walking in patients with cerebral palsy
Фотографии:

ˑ:
Postgraduate student S.D. Korshunov2
Ph.D., Associate Professor K.V. Davlet’yarova2
Professor, Dr.Med. L.V. Kapilevich1
1National Research Tomsk State University, Tomsk
2National Research Tomsk Polytechnic University, Tomsk
Keywords: walking, locomotion, movement disorders, electromyography, antagonist muscles.
Introduction. Cerebral palsy (CP) is a severe neurological disease that substantially limits child’s vital activity. First of all, it leads to movement disorders [3].
An important physiological indicator of locomotor stereotypes is the nature of the bioelectrical activity of muscles during their performance [1, 2]. There are many works dedicated to the analysis of motor disorders in children with cerebral palsy, but most of them are focused on the description of the pathogenetic mechanisms [4]. At the same time existing pathological motor stereotypes can be the basis for the formation of new motor skills which will lead to an increase in the motor activity of a child and have a good rehabilitation effect [4].
Objective of the research was to study the peculiarities of bioelectrical activity of muscles when walking in patients with cerebral palsy.
Materials and methods. Twenty children (12 boys and 8 girls) aged from 8 to 12 years, suffering from cerebral palsy, including 10 children capable of walking on their own and 10 children capable of handrail-supported walking only were examined. The reference group consisted of 10 healthy children (6 boys and 4 girls) of the same age. All the subjects walked on an electric treadmill on a level surface. The bioelectrical muscle activity was measured using the digital EMG and EP system Neuro-MEP-4. The electrodes were placed on the following muscles (on the right and left-hand sides): calf muscle (medial head); lateral vastus muscle; biceps muscle of thigh; rectus muscle of back. Factual data are presented in the form of “mean ± error of mean” (М±m). The significance of inter-group differences was assessed using the nonparametric Mann-Whitney test.
Results and discussion. The table shows that parameters of the interference EMG of the tested muscles of patients with cerebral palsy who can walk on their own and of those walking with support are considerably different. We observe reduction of the maximum oscillation amplitude in the calf muscle and an increase of its mean amplitude in the children capable of unsupported walking. Changes of the calf muscles' bioelectrical activity in children walking with support only are of largely opposite nature: minor multidirectional amplitude variations combined with a significant increase in the frequency of oscillations and a significant reduction of the amplitude and frequency parameters compared with the reference group. In terms of the lateral vastus muscle (extensor of the knee joint) the changes are quite similar: the bioelectrical activity of the biceps muscle of thigh (posterior muscle group) hardly differed from the reference values.
Characteristics of the bioelectrical activity of the rectus muscles of the back significantly differed from those in the reference group. In both of the groups of children with cerebral palsy we observe an increase in the maximum and total oscillation amplitudes. Mean frequency significantly reduced in the group of children capable of unsupported walking and increased in the group of children who can walk only with support.
Results of the turns and amplitudes analysis presented in Figures 1-3 were particularly illustrative. The main differences of the dynamic stereotype of walking in the children with cerebral palsy according to the electromyographic analysis are as follows:
– the most significant changes are in the calf muscles' bioelectrical activity. At the same time we observed in children capable of unsupported walking a phenomenon of hyper synchronization – a significant increase of the amplitude of oscillations in combination with a decrease in frequency. A “cloud” of turns shifts upwards, reflecting involvement of the central compensatory mechanisms. There is no synchronization in children walking with support only: the amplitude of oscillations decreases, and the frequency increases significantly. A “cloud” of turns shifts to the right, indicating the prevalence of myogenic regulatory mechanisms;
– excessive activity of rectus muscles of the back is observed in both of the groups of the patients with cerebral palsy in comparison with the reference group. At the same time in the children capable of unsupported walking a phenomenon of synchronization (a reduction in frequency with increasing amplitude and a shift of one of the “clouds” of turns upwards) was observed. Excessive activity of this muscle group was not accompanied by synchronization in the group of children walking with support only (the frequency of oscillations increased), the “cloud” of turns shifted horizontally to the right;
– activity of the posterior muscle group of thigh decreased slightly in both of the groups of children with cerebral palsy, activity of the anterior muscle group of thigh increased in both of the groups but the increase was more pronounced in children capable of unsupported walking.
Conclusion. The dynamic stereotype of walking in children with cerebral palsy is distinguished by excessive involvement in locomotions of calf muscles and rectus muscles of the back, with central mechanisms of hypersynchronization of activity of motor units being the main adaptation mechanism in the group of children who can move themselves. Exercises for these muscle groups can be included in the rehabilitation complex.
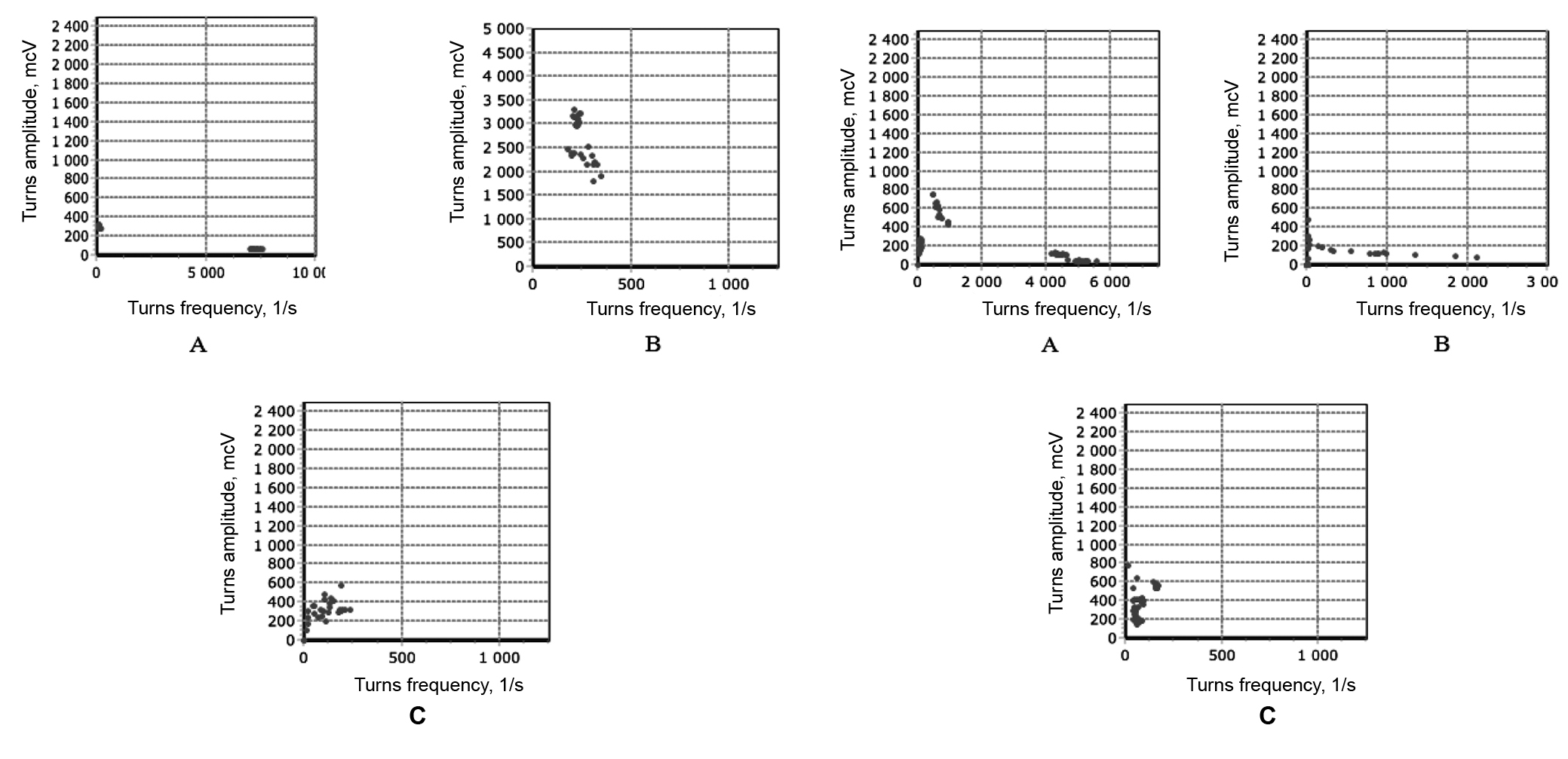
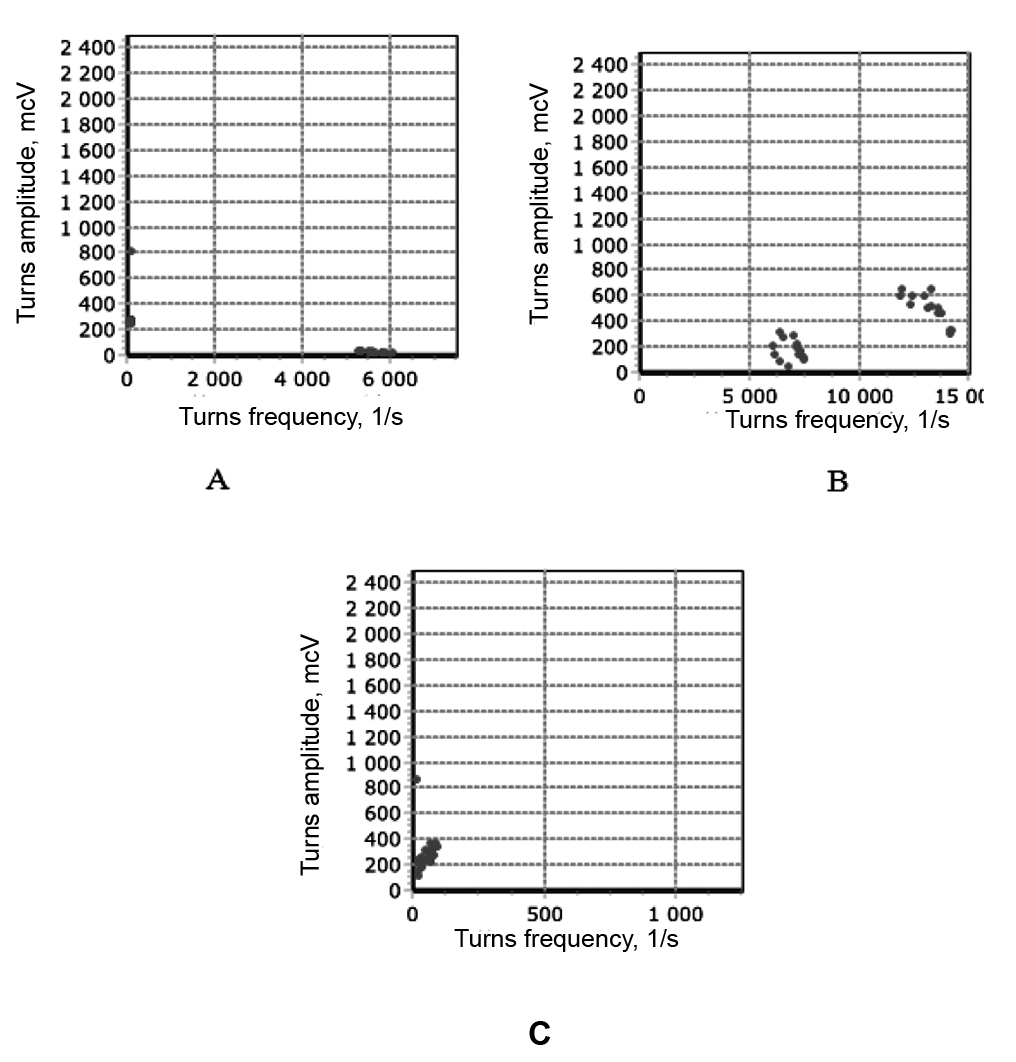
Diagrams of turns and amplitudes analysis of electromyograms:
1 – calf muscle (medial head), 2 – lateral vastus muscle, 3 – rectus muscle of back.
А – patients with cerebral palsy walking with support, B – patients with cerebral palsy walking on their own, C – healthy children
Parameters of bioelectrical activity of skeletal muscles in patients with cerebral palsy and in the reference group when walking
|
Parameters
MUSCLES |
Max amplitude, mcV |
Mean amplitude, mcV |
Total amplitude, mV/s |
Mean frequency, 1/s |
Amplitude/ frequency, mcV×s |
|||||||||||
|
Walking with support (CP) |
Walking without support (CP) |
Healthy |
Walking with support (CP) |
Walking without support (CP) |
Healthy |
Walking with support (CP) |
Walking without support (CP) |
Healthy |
Walking with support (CP) |
Walking without support (CP) |
Healthy |
Walking with support (CP) |
Walking without support (CP) |
Healthy |
||
|
Calf muscle (medial head) |
Left leg |
11803±1005* |
2825±389* |
10089±977 |
184±35* |
844±164* |
405±57 |
863±156* |
268±44* |
195±30 |
4725±630* |
652±98* |
1275±100 |
3.7±0.9* |
20±3.5* |
8.5±1.8 |
|
Right leg |
10300±1115* |
3636±567* |
7129±913 |
447±84* |
869±150* |
238±32 |
1001±200* |
267±51* |
131±25 |
2165±380* |
285±40* |
1254±97 |
1.9±0.5* |
77.3±15* |
10.7±2.1 |
|
|
Lateral vastus muscle |
Left leg |
2176±402* |
10610±887* |
5367±612 |
173±28 |
899±145* |
229±28 |
372±38 |
520±105* |
175±41 |
4722±720* |
1025±115* |
2664±180 |
23.5±4.2* |
18.9±3.3* |
54.9±7.4 |
|
Right leg |
4005±565 |
11314±1300* |
3162±420 |
481±70 |
373±65 |
341±55 |
2584±352* |
179±25 |
75±10 |
4482±490* |
1412±230 |
1167±247 |
21.8±3.2* |
9.6±1.1 |
6.8±0.9 |
|
|
Biceps muscle of thigh |
Left leg |
1205±120 |
2258±370 |
2824±355 |
348±42 |
400±77 |
403±62 |
44±8 |
101±15 |
86±11.5 |
308±62 |
634±79 |
1112±135 |
4.9±0.2 |
79.3±7.1 |
210.9±25.0 |
|
Right leg |
1205±190 |
2949±370 |
1964±220 |
348±45 |
343±40 |
336±42 |
44±7 |
89±8.5 |
11±1.9 |
308±48 |
248±25 |
47±4 |
4.9±0.75 |
42.8±4.9 |
23.8±2.9 |
|
|
Rectus muscle of back |
Left |
13002±1420* |
9180±990* |
5147±778 |
341±45 |
1347±175* |
162±25 |
2767±310* |
885±95* |
230±27 |
6524±750* |
1154±142* |
4647±620 |
2.9±0.35* |
10.3±1.5* |
28.3±3.1 |
|
Right |
5521±620 |
7362±750* |
4687±510 |
175±20 |
1486±160* |
227±25 |
570±69* |
1751±190* |
222±30 |
4011±420* |
2237±255* |
3026±340 |
2.5±0.3* |
12.9±1.3* |
36.7±4.1 |
|
* – significance of differences from the reference group (p<0.05).
The work was supported by the Russian Foundation for Humanities №15-16-70005.
References
- Illarionova A.V. Osobennosti vnutrimyshechnoy i mezhmyshechnoy koordinatsii pri dozirovanii usiliy v usloviyakh neustoychivogo ravnovesiya (Specifics of intramuscular and intermuscular coordination when dosing load under unstable equilibrium) / A.V. Illarionova, L.V. Kapilevich // Teoriya i praktika fizicheskoy kul’tury. – 2014. – № 12. – P. 44–46.
- Kapilevich L.V., Guzhov F.A., Bredikhina J.P., Ilyin A.A. Fiziologicheskoe obespechenie tochnosti i koordinatsii dvizheniy v usloviyakh neustoychivogo ravnovesiya i podvizhnoy tseli (Physiological maintenance of accuracy and coordination under unstable equilibrium and moving target) / D.V. Kapilevich, F.A. Guzhov, J.P. Bredikhina, A.A. Ilyin // Teoriya i praktika fizicheskoy kul’tury. – 2014. – № 12. – P. 22–24.
- Osokin V.V. Evolyutsiya predstavleniy o detskom tserebral’nom paraliche (Evolution of cerebral palsy concepts) / V.V. Osokin // Sovremennaya nauka: aktual’nye problemy i puti ikh resheniya. – 2014. – №9.
- Marret S. Pathophysiology of cerebral palsy // S. Marret, C. Vanhulle, A. Laquerriere. –HandbClin Neurol. 2013;111:16976.
Corresponding author: kapil@yandex.ru

