
Individualized de-adaptation risk forecasts in academic physical education process
ˑ:
Dr. Biol. M.V. Postnova1
PhD, Associate Professor Yu.A. Shatyr1
I.V. Ulesikova2
Dr. Biol., Professor A.B. Mulik3
1Volgograd State University, Volgograd
2S.M. Kirov Military Medical Academy, Moscow
3Institute of Toxicology of Federal Medico-Biological Agency (IT FMBA), Moscow
Keywords: physical education service individualization, adaptive responses, physical load, de-adaptation risk, combined unspecific bodily reactivity.
Background. National health statistics for the last few years reports an alarming growth in the sudden deaths of trainees during standard physical education practices. Modern physical load rating standards for the physical education service at the national secondary/ vocational/ higher education establishments were designed to regulate the physical process intensity and exercises for three academic health groups (main, preparatory and special) on a gender- and age-specific basis. It should be acknowledged, however, that the existing physical load individualization system is fairly efficient only in application to the main health group (MHG). In the prior qualifications for the main and preparatory health groups, the relevant medical personnel are governed by the basic health and physical development criteria having their natural limitations – since such qualifications unsupported by extensive tests may not always be accurate enough to avoid/ prevent the further individual de-adaptation and overstress risks that may result in stress-specific health disorders in some cases [2,4].
Our prior studies demonstrated benefits of the combined unspecific reactivity rating tests for the individual adaptability assessment and de-adaptation risk exposure rating purposes in the regular physical education service.
Objective of the study was to develop, on a sound theoretical basis, and test benefits of an individualized de-adaptation risk assessment model applicable in the academic physical education process.
Methods and structure of study. The first stage of the study was geared to find logics in the individual combined unspecific bodily reactivity (ICUBR) profiles. Sampled for this stage of the study were the 18-25 year-old formally healthy students of Volgograd State University (n=100, with equal gender shares). The individual combined unspecific bodily reactivity was rated by the pain tolerance thresholds (PTT) using an Ugo Basile analgesiometer (Italy made) that tests the nociceptive sensitivity by rating the reflective wrist withdrawal move from the tolerant-temperature beam acting on the distal phalange backside, with the move time (s) assumed indicative of the pain tolerance thresholds [5]. Thus the high and average individual combined unspecific bodily reactivity rates correspond to the low and average pain tolerance thresholds rates, respectively.
At the second stage we run the adaptation stress tests in the practical physical education sessions based on the pre-training individual combined unspecific bodily reactivity rates [1]. Sampled for this stage of the study were 18-20 year old first-year students (n=46) qualified with the main health group who self-rated their wellbeing as fair and free of expressed fatigue. Prior and after every training sessions the trainees were tested for individual combined unspecific bodily reactivity, blood pressure and HR; with their wellbeing and fatigue rated by formal questionnaires. [1,2]. The physical trainings were run as required by the Volgograd State University curriculum with the first-module 3000/ 2000m (male/ female) cross-country race tests.
And the third stage of the study was designed to develop a disease-prevention individualized de-adaptation risk assessment algorithm for application in the standard academic physical education process.
Study findings. Based on the individual combined unspecific bodily reactivity rates versus the maximal/ minimal pain tolerance thresholds rates (varying from 3s to 41s) and relevant test rate ranges and frequency distribution rages obtained at the first stage of the study, we grouped the sample into the high-, average- and low individual combined unspecific bodily reactivity classes, with the class interval equal to λ = (41 – 3) / (1 + 3,32 lg100) = 5, and the bottom limit of the first class equal to x = 3 – 5/2 = 0,5. Based on the classified test rate ranges, we produced the following diagram of the pain tolerance thresholds test rates for the individual combined unspecific bodily reactivity classes: see

Figure 1. Pain tolerance thresholds test rates for the individual combined unspecific bodily reactivity classes: distribution diagram
Further analysis of the biometric test data showed normality of the PST distribution for the sample (n = 100). Thus the pain tolerance test ranges were found fairly wide albeit symmetric, with the peaks in the middle of each range and gradual decreases towards the class limits – that may be interpreted as the general biological logic of this physical quality. It should be noted that the individual combined unspecific bodily reactivity test rates found gender-unspecific. The analysis demonstrates efficiency of the pain tolerance thresholds rating tests for the individual combined unspecific bodily reactivity rating and classifying purposes. The data mined at the second stage of the study made it possible to profile and classify the individual adaptive responses in the standard physical education process versus the primary individual combined unspecific bodily reactivity rates: see Figure 2.
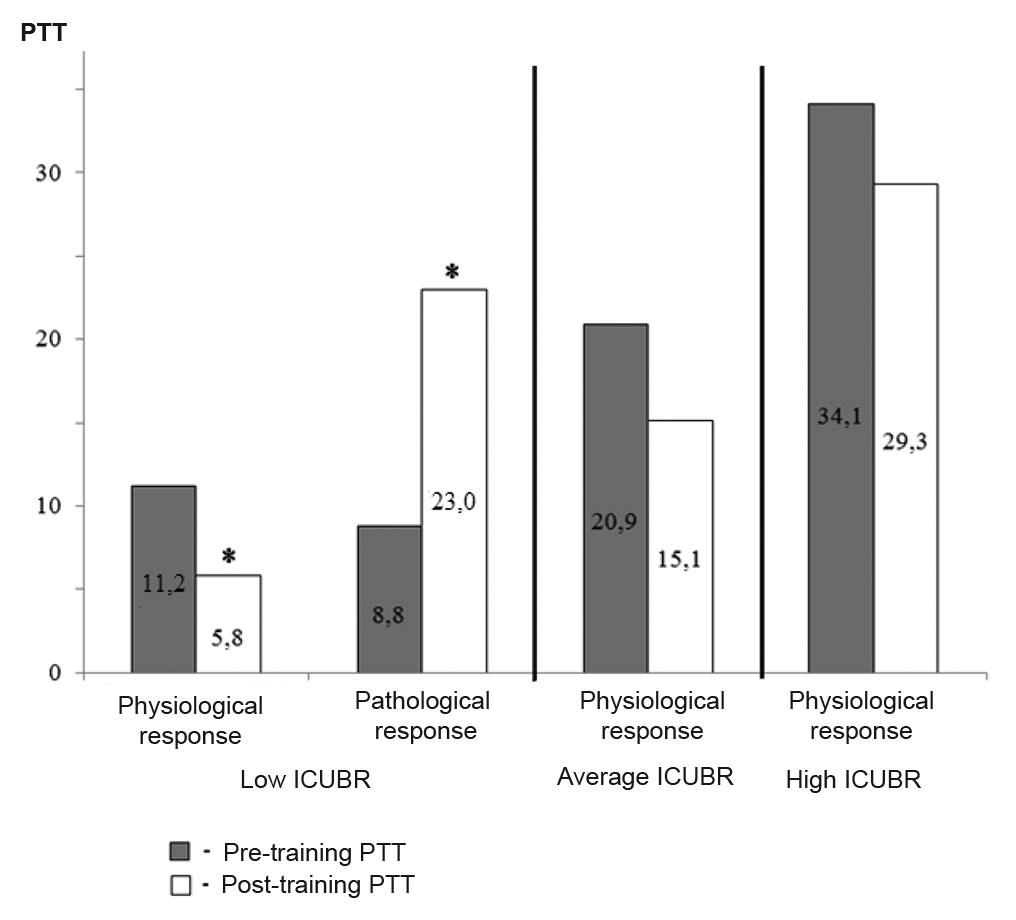
Figure 2. Pain tolerance thresholds variations for the ICUBR classes
Note: *statistically significantly (р<0.05) pre- versus post-training pain tolerance thresholds variations
The average- and low- individual combined unspecific bodily reactivity groups were tested with the physiologically normal adaptive responses (with the post-training pain tolerance thresholds falling); whilst the high-individual combined unspecific bodily reactivity group was found different in this aspect, with 25% of the group (3 females and 2 males) tested with pathological responses to the standard physical education trainings indicative of the low stress tolerance [3] and acute fatigue and de-adaptation, as was substantiated by the medical examination data as well [1].
At the third stage of the study, we developed a de-adaptation risk assessment algorithm applicable in the prior tests of the MHG qualifiers. We recommend the standard medical examination and test procedure being complemented by the pain tolerance thresholds tests followed by individual combined unspecific bodily reactivity grouping tests and analyses, with the individual combined unspecific bodily reactivity actually rated in the pain tolerance thresholds values (seconds) produced by an analgesiometer system: see Table 1 hereunder. Then the students qualified with the high-individual-combined-unspecific-bodily-reactivity (high-risk) group shall be tested for the response rates to profile their static/ dynamic reactivity on an all-round basis.
Table 1. Correlation of the pain tolerance rates with the individual combined unspecific bodily reactivity rates
|
Pain tolerance threshold, s |
||
|
High-ICUBR group |
Average-ICUBR group |
Low-ICUBR group |
|
0,5-15,4 |
15,5 – 30,4 |
30,5-45,5 |
For the individual combined unspecific bodily reactivity grouping purposes, the analysts shall rate the pre- and post-training (minimal and maximal) blood pressure (systolic and diastolic BPmin and BPmax), heart rates (HRmin and HRmax), with the tests designed as follows: quiescent-state tests (after at least 5min rest); and post-training tests, with the training limited by 10 squats per 10s; and with SBP calculated as (2×DBP)+SBP)/3 (DBP and SBP meaning the diastolic and systolic pressures, respectively).
The integrated bodily reactivity shall be computed in the following three stages. Stage one calculation rates the bodily reactivity (BR) by HR as follows: BRhr= (HRmax - HRmin)/ PTT. Stage two calculation rates the bodily reactivity (BR) by BP as follows: ВРap= (SBPmax - SBPmin)×2)/ PTT. And the stage two calculation produces the integrated bodily reactivity index as follows: IR=(BRhr+ BRap)/2.
Individuals tested with the IR rates varying within 5-minus, 5-10 and 10-plus points shall be ranked with the low- average- and high-IR groups (exposed to low, average and high de-adaptation risks), respectively. The individuals tested with the high de-adaptation risks shall be qualified with the special health groups regardless of how good the health test data produced by the standard medical examinations and tests are.
Conclusions
1. High individual combined unspecific reactivity rates are associated with the high risks of de-adaptation in the standard physical trainings.
2. Tests to profile the cardiovascular system performance versus the pain tolerance threshold rating tests give the means to assess the individual stress exposure in the standard physical education process.
3. Individuals tested with the high de-adaptation risks shall be qualified with the special health groups regardless of how good the health test data produced by the standard medical examinations and tests are – to reasonably customize the training process to their health conditions and avoid the risks of their adaptive physiological responses running beyond the norm.
References
- Velitchenko V.K. Fizkultura bez travm [Physical education without injury]. Moscow: Prosveshchenie publ., 1993, 128 p.
- Vorobyev L.V. Porogovaya ChSS kak kriteriy bezopasnykh nagruzok na serdtse [Threshold heart rate as criterion of safe heart loads]. Uspekhi sovremennogo estestvoznaniya, 2014, no. 2, pp. 7-11.
- Garkavi L.Kh. Aktivatsionnaya terapiya. Antistressornyie reaktsii aktivatsii i trenirovki i ikh ispolzovanie dlya ozdorovleniya, profilaktiki i lecheniya [Activation therapy. Anti-stress activation and training reactions and their use for recovery, prevention and treatment]. Rostov-on/D.: RU publ., 2006, 256 p.
- Zaytsev A.A. Metodologiya normirovaniya nagruzok v fizicheskoy kulture [Methodology of load regulation in physical education]. Izvestiya Baltiyskoy gosudarstvennoy akademii rybopromyslovogo flota: psikhologo-pedagogicheskie nauki, 2013, no. 4 (26), pp. 48-53.
- Mulik A.B., Postnova M.V., Mulik Yu.A. Uroven obschey nespetsificheskoy reaktivnosti organizma cheloveka [Level of general non-specific reactivity of human body]. Volgograd: VS publ., 2009, 224 p.
- Milashechkina E.A., Jandarova T.I. Physical progress rates of special health group students diagnosed with cardiovascular system disorders versus their physical activity rates. Theory and Practice of Physical Culture, 2018, no. 4, 6 p.
- Serikov S.G., Serikov G.N. Health promotion role of physical education in university learning process. Theory and Practice of Physical Culture, 2016, no 5, 2 p.
- Popova T.V., Koryukalov Y.I., Kourova O.G., Dovbiy I.P. Adaptation of sporty students to academic load under fatigue and mental stress. Theory and Practice of Physical Culture, 2017, no. 4, 17 p.
- Corresponding author: fizkult@teoriya.ru
Abstract
Objective of the study was to develop, on a sound theoretical basis, and test benefits of an individualized de-adaptation risk assessment model applicable in the academic physical education process. Sampled for the model tests were the 18-20 year-old students of Volgograd State University (n=146). The first stage of the study was geared to find logics in the individual combined unspecific bodily reactivity profiles. The second stage included the adaptation stress rating tests and analyses versus the individual combined unspecific bodily reactivity rates. And the third stage of the study was designed to develop a disease-prevention individualized de-adaptation risk assessment algorithm for application in the standard PR trainings. The study data and analyses showed benefits of the new individualized de-adaptation risk assessment model for the academic physical education process.

