
Future teacher’s health values and motivations building physical education model
ˑ:
Dr.Med., Professor T.V. Karaseva1
PhD O.V. Turbachkina1
PhD, Associate Professor A.M. Loshchakov2
1Ivanovo State University, Ivanovo
2Ivanovo State Medical Academy, Ivanovo
Background. Academic physical education is intended to not only ensure the vital motor skills building, but also train a polite, educated, physically and intellectually developed and socially active individual [2]. Motivations for physical trainings are viewed as an important and absolutely necessary condition for the formation of a future teacher's health culture by means of physical education. The academic education period is known to be the best time to build motivations for a healthy, long and successful professional service and healthy lifestyle [1]; with the academic physical education service playing a consolidation role since every physical education value contributes to a health agenda.
Objective of the study was to test by experiment benefits of of a new health-centered physical education model geared to effectively develop health values and motivations in the future education specialists.
Results and discussion. The sample progress in the health values and motivations were rated by the pre- versus post-experimental tests in the new health-centered physical education model piloting experiment under the academic physical education curriculum. The students’ health values and motivations were self-rated by a Future Teacher Health Culture test of our own design [3]. Sampled for the model testing experiment were Shuya Branch students of Ivanovo State University (n=190) aged 17-24 years split up into Experimental (EG) and Reference (RG) Groups of 95 people each (75 females and 20 males).
To secure good progress in the values-and-motivations component of the academic health culture, we complemented the valid physical education theory course by lectures on hygiene and health protection basics, with a special emphasis on motivations for healthy lifestyles and physical education-driven health cultures. Practical physical education sessions were complemented by health-prioritizing physical practices with self-controlled workloads and the injury prevention and natural environment sensitive elements. Given in Table 1 hereunder are the values-and-motivations rating criteria applied for the health culture progress tests of the future education specialists, used as a basis for the questionnaire survey form.
Table 1. Values-and-motivations component rating criteria in the future teacher’s health culture rates|
Component |
Rating criteria |
Rate level |
||
|
High |
Mean |
Low |
||
|
Values-and-motivations |
Attitude to academic physical education, physical education specialty and research |
Lively interest in every theoretical and practical issue of hygienic education, healthy lifestyles and health culture |
Fragmented interest in some issues of hygienic education, healthy lifestyles and health culture |
Poor interest in issues of hygienic education, healthy lifestyle and health culture viewed as largely unimportant for future service |
|
Attitude to the own hygienic education, healthy lifestyle and health culture |
Sustainable genuine need for hygienic education, healthy lifestyle and health culture as the personality progress and career success elements; and good motivations for a healthy lifestyle |
Occasional natural need for hygienic education, healthy lifestyle and health culture – mostly under external pressure; and unstable motivations for a healthy lifestyle |
Poor internal motivations for hygienic education, healthy lifestyle and health culture in the physical education process; and learning progress only under external pressure |
|
|
Tested values and motivations |
High-level rates |
t |
p |
|
|
Pre-experimental tests, % |
Post-experimental tests, % |
|||
|
Physical activity motivations |
41,05 |
62,11 |
2,97 |
< 0,05 |
|
Healthy diet motivations |
46,32 |
86,32 |
6,44 |
< 0,05 |
|
Immunity to unhealthy habits |
42,11 |
92,63 |
8,82 |
< 0,05 |
|
Healthy family motivations |
2,11 |
7,37 |
1,72 |
> 0,05 |
|
Motivations for healthy education process |
38,95 |
74,74 |
5,34 |
< 0,05 |
|
Motivations for positive peer relationship |
35,79 |
64,21 |
4,07 |
< 0,05 |
|
Motivations for positive relationship with the faculty |
27,37 |
76,84 |
7,86 |
< 0,05 |
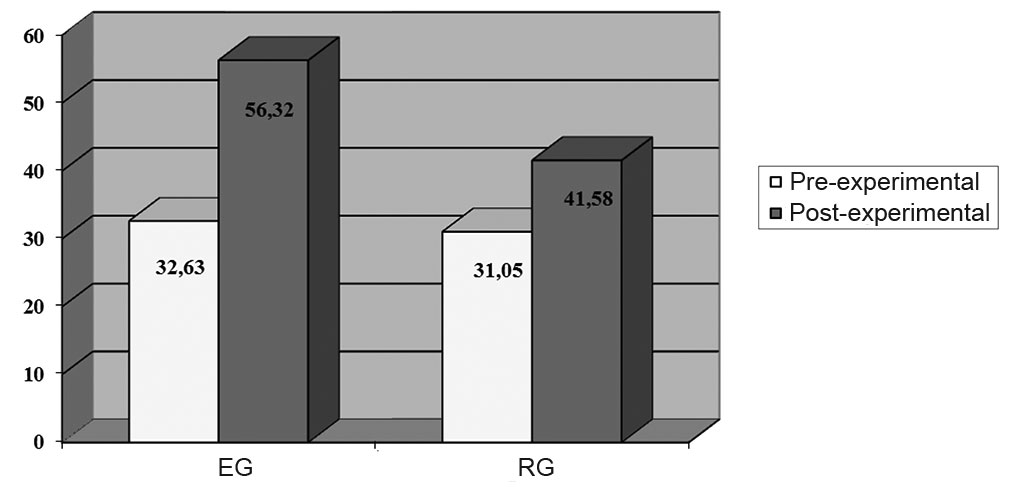
Figure 1. Progress of the high-level values-and-motivation component in the EG and RG rated by the pre- versus post-experimental tests
The high-level values-and-motivation component in the RG was tested to make progress from 31.05% to 41.58% as verified by the pre- versus post-experimental tests. The EG and RG progress analysis showed the EG progress being significantly ((р<0.05) higher versus the RG as demonstrated by the growth from virtually the same pre-experimental group test level of 32.63% and 31.05% to the post-experimental 56.32% and 41.58% in the EG and RG, respectively.
In the values-and-motivations component building process special attention was given to the trainees’ motivations for health basics learning, health culture and healthy lifestyle. High motivations in these domains are known to facilitate progress of the cognitive component at the next stage of the health culture development educational process.
The EG and RG subgroups with high motivations for health basics learning made a significant (p≤0.05) progress from 25.4% to 59.6% and from 24.24% to 40.43%, respectively, as found by the pre- versus post-experimental tests. Despite the virtually the same pre-experimental rates (25.4% and 24.24%, respectively), progress of the EG versus RG subgroup was tested significantly (p≤0.05) higher (to 59.6% and 40.43%, respectively).
Given on Figure 2 hereunder is the EG and RG pre- versus post-experimental healthy lifestyle and health culture motivations progress test rates.
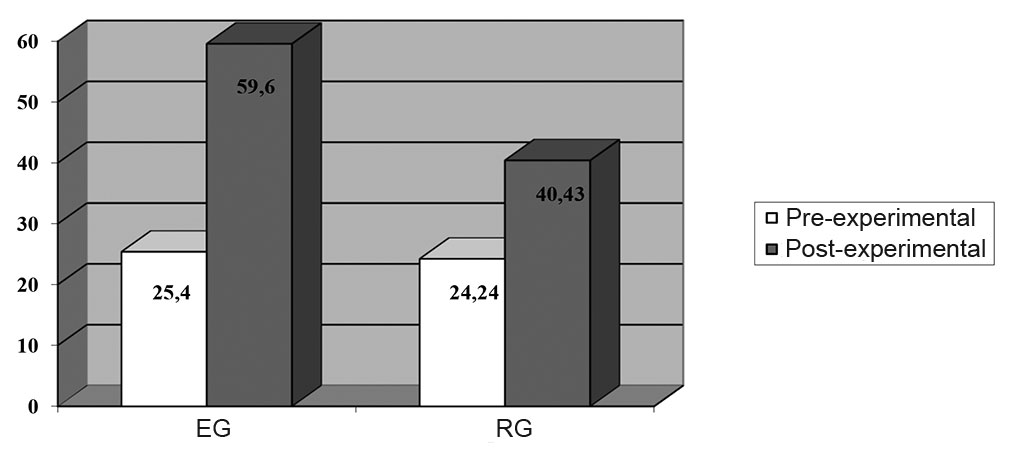
Figure 2. Pre- versus post-experimental healthy lifestyle and health culture motivations progress test rates in the EG and RG
The health culture values-and motivations component rating tests found the new health-centered physical education model rated satisfactory by 35.79% and 33.68% of the EG and RG in the pre-experimental tests – versus 58.95% and 38.95% in the post-experimental tests, respectively. Negative ratings of the model were tested to fall from 30.53% to 15.79% and from 29.47% to 23.16% in the EG and RG, respectively.Conclusion. The new health-centered physical education model under the academic physical education curriculum with an emphasis on the hygienic issues was tested beneficial as verified by the progress of the sample in the values-and-motivations component of the health culture. We used the model piloting experience and tested practical education tools to develop a training program component for the academic Physical Education and Healthy Lifestyle Basics discipline as required by the new-generation education standard.
References- Lisitsyn Yu.P. Zdorovye naseleniya i sovremennye teorii meditsiny [Public health and modern theories of medicine]. Moscow: Meditsina publ., 1982, 326 p.
- Turbachkina O.V. Sovershenstvovanie sistemy fizicheskogo vospitaniya studentov v tselyakh formirovaniya kultury zdorovya [Efforts to improve academic physical education system to form health culture]. PhD diss.. Moscow, 2012, 135 p.
- Turbachkina O.V. Formirovanie kultury zdorovya: upravlenie kachestvom fizicheskogo vospitaniya studentov [Health culture cultivation process: academic physical education quality management]. Shuya, 2012. 168 p.
Abstract
Academic physical education is intended to not only ensure progress in the core motor skills, but also train a polite, educated, physically and intellectually developed and socially active individual. Due motivations for physical training are viewed as an important and absolutely necessary condition for the future teacher's health culture formation by means of physical education. The article analyzes benefits of a new health-centered physical education model geared to effectively develop health values and motivations in the future education specialists. The model includes theoretical, practical, methodological and progress test components making an emphasis on the health protection and improvement aspects with reasonable revisions of the traditional axiological and theoretical education elements. Due priority in the model design was given to the motivations building aspects since they are indispensable for any health agenda and culture. The students’ health values and motivations were self-rated by a Future Teacher Health Culture test. Sampled for the model testing experiment were the Shuya Branch students of Ivanovo State University (n=190) split up into Experimental (EG) and Reference (RG) Groups. The study data and analyzes showed benefits of the new health-centered physical education model as verified by the sample progress in the health values and motivations rating tests.

